 Alice Varley, one of our Data Impact Fellows, explores why access to mental healthcare matters, how a new composite measure can better capture accessibility to mental healthcare, and why gaps in available data still limit our ability to address mental health inequalities.
Alice Varley, one of our Data Impact Fellows, explores why access to mental healthcare matters, how a new composite measure can better capture accessibility to mental healthcare, and why gaps in available data still limit our ability to address mental health inequalities.
Why should you care about access to mental healthcare?
Unlike many other health conditions, mental health problems and disorders are something that many of us will struggle with at some point in our lives. In fact, 1 in 6 of us experience symptoms of anxiety and depression each week. Despite this, as many as 61% of adults with mental health conditions don’t access treatment.
Improving access to mental healthcare is fundamental in addressing this lack of treatment, and to ultimately work towards improving wider mental health inequalities in society.
Why do we need a composite measure of mental healthcare accessibility?
To achieve these aims, we need to first understand how easy it is to access mental health services. In doing this, we need to make sure to encompass diverse concepts related to both the physical and social factors that impact this mental healthcare accessibility. Accessibility itself in this context represents the potential or opportunity to receive mental healthcare as well as how easy it is to get appropriate treatment.
As a non-communicable disease, there is much more emphasis on the social aspects affecting mental healthcare access, such as awareness of issues and stigma. This means that there are multiple factors to reconcile when considering how to assess access levels for mental health treatment services.
I responded to this need for further knowledge by developing a composite score of mental healthcare accessibility across neighbourhoods in Liverpool. More specifically, these neighbourhoods are small geographic areas known as lower-layer super output areas, or LSOAs. I did this by creating separate scores addressing spatial and social accessibility (respectively) and then combining these into a metric that embodies a holistic measure of mental healthcare accessibility.
Spotlight on the data
Mersey Care NHS Foundation Trust, GridReferenceFinder.com, and Ordinance Survey CodePoint Open enabled me to create localised point data to represent key locations for Mersey Care. However, it is very laborious to do this for multiple NHS trusts (as I am currently doing!).
I used data from OpenStreetMap and Bus Open Data Service to create street networks, enabling me to calculate travel times using different modes of transport. These resources were easy to use and very helpful.
Finally, I used various data from the Consumer Data Research Centre (now the Geographic Data Service), Office for National Statistics, and the 2021 Census to examine barriers to accessibility arising from sociodemographic characteristics. These data were fairly straightforward and easily accessible, however some variables might not have been available in the right format, e.g. one at household level and one at an individual level, which requires some manipulation of the data.
Creating a composite measure: my thoughts so far
Figure 1 is a map of the composite accessibility score calculated for LSOAs in Liverpool. Notice how the darker blue values, which correspond to lower mental healthcare accessibility, coincide with some of the most historically deprived areas.
Figure 1: Map of composite accessibility score for LSOAs in Liverpool.
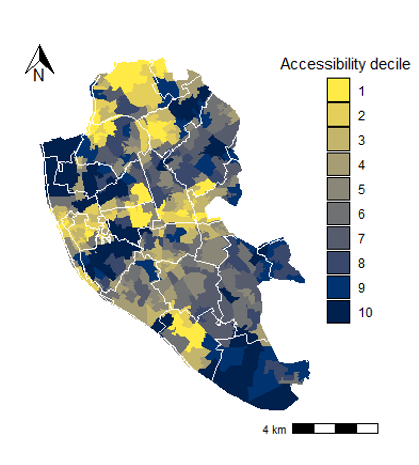
Note that higher values / darker regions represent poorer mental healthcare accessibility scores. Larger version
But that’s not all we can learn!
A lack of data can limit health inequality monitoring
However, this composite score was limited by the lack of openly available data. To calculate the spatial accessibility scores, I used a method called enhanced two-step floating catchment area. This involves the integration of both supply (healthcare providers) and demand (patients) measurements.
Whilst this was relatively straightforward for the demand side, which I approximated using the population size of each neighbourhood, there was no available data (as far as I was aware) to represent available resources from healthcare systems. This information would only need to be relatively simple, such as the number of beds or healthcare professionals working in a particular location, yet it would make the overall mental healthcare accessibility measure much more accurate.
Responsible use of data and the impact of organisational infrastructure
Of course, in healthcare data there is the concern for confidentiality, which is arguably more prominent than in many other areas of social science. That said, this confidentiality is predominantly related to the patients themselves, rather than workforce data, so whilst it is a valid concern, it is less relevant here. In addition, it would also be beneficial to be able to work with more exact figures of the number of patients, but this is less important than gaining access to supply-level data, such as workforce numbers at different NHS sites.
Additionally, there may be teams working across multiple sites, meaning that it may not be possible to pin down accurate numbers on numbers of healthcare professionals working at a particular location.
The number of beds available is a useful alternative to this, even if this misses crucial information such as how long patients stay and how long they may have to wait to be admitted. Focusing on beds as a supply measurement also limits analysis, requiring me to solely focus on inpatients, and exclude day patients and outpatients attending for appointments.
Thus, whilst it is evident that the provision of more data about the availability and capacity of services would improve measures around mental healthcare accessibility, there are several considerations we need to be aware of first.
Key takeaways
To create a comprehensive mental healthcare accessibility metric, we need to balance the need for more data with approaches that reflect the sensitive nature of what we are measuring. This is no simple feat, but could include making supply data, such as staff and bed numbers in particular treatment sites, more readily available.
Ultimately, there is a need for publicly available supply data to make more accurate and impactful metrics, which is fundamental in enabling accurate and insightful monitoring of health inequalities such as accessibility of mental healthcare.
About the author
Alice is a second-year PhD student at the Geographic Data Science Lab (University of Liverpool).
In partnership with Mersey Care NHS Foundation Trust, her research explores mental health inequalities in Liverpool. Using quantitative methods, the project aims to investigate the determinants and prevalence of mental health inequalities, revealing how various spatial, demographic, and socioeconomic factors interact with these observed disparities. Ultimately, the focus is on improving services and interventions through tackling inequalities, using the evidence generated through this research.
Her PhD programme involves an integrated MSc over the first two years, so her research is still in its very early stages.
One week to go

If you are already registered and looking forward to Perspectives on Engagement and Impact, we can’t wait to welcome you to Manchester on February 11!
If you haven’t signed up yet, please register your interest and we will be in touch if a spot becomes available.
Comment or question about this blog post?
Please email us!